
Triglycerides: The Goldilocks Problem
Not too high. Not too low.
Triglycerides have become the lipid we love to hate.
High? Bad.
Lower? Better.
Lowest possible? Even better.
That’s simple, reassuring - and incomplete.
Triglycerides are often discussed as if they’re metabolic waste, something to suppress aggressively. But biologically, triglycerides are part of the system that keeps lipids contained, buffered, and well-behaved. Treating them as disposable misses what they actually do - both in circulation and inside cells, including in the brain.
If this sounds familiar, it should. I made a similar point in an earlier post on statins: lipid biology rarely rewards absolutism. “Lower” can be helpful - until it isn’t. Triglycerides may be the clearest example of where that line gets crossed.
And for anyone thinking about Alzheimer’s risk, APOE genotype, or aging physiology, this nuance matters.
Triglycerides aren’t just a blood number
Yes, fasting triglycerides largely reflect triglyceride-rich lipoproteins (mostly VLDL). And yes - chronically elevated triglycerides in midlife often signal insulin resistance, excess remnant particles, fatty liver, and higher cardiovascular risk.
That part of the story is real.
But triglycerides are also the backbone of lipid droplets - dynamic intracellular organelles found in liver, muscle, immune cells, and importantly, astrocytes in the brain. Lipid droplets are not passive fat storage. They are a containment system.
They exist to:
safely sequester fatty acids
prevent lipotoxicity
buffer oxidative stress
supply energy during demand
protect mitochondria from overload
In other words, triglycerides are one of the ways biology keeps lipids from misbehaving.
Lipid droplets need triglycerides to stay functional
Here’s where things get interesting - and where the “lower is better” narrative starts to wobble.
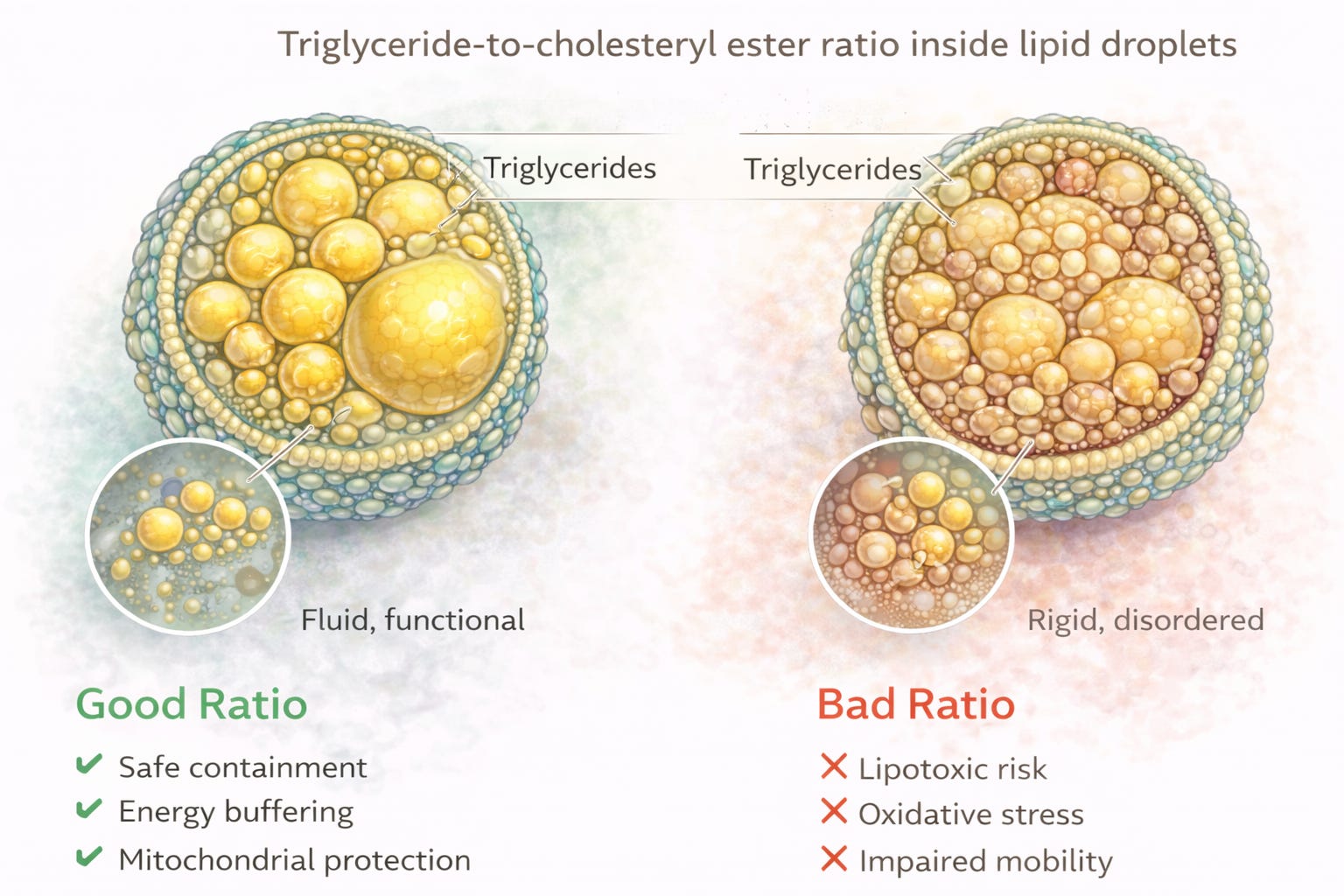
Recent cellular work shows that the ratio of triglycerides to cholesteryl esters inside lipid droplets affects their physical state. When triglycerides are depleted—such as during sustained lipolysis or severe energy restriction - lipid droplets can undergo phase transitions, shifting toward more rigid, liquid-crystalline states.
Why does that matter?
Because fluid lipid droplets behave differently than rigid ones. Organization matters. Mobility matters. And rigidity tends to show up under metabolic stress.
Triglycerides, in sufficient proportion, help keep lipid droplets fluid and functional. This is not about excess. It’s about balance.
That idea aligns surprisingly well with broader work on phase separation and membrane dynamics, a conceptual framework explored by researchers like Doris Loh and discussed in a previous post. The takeaway isn’t that triglycerides are “protective” in isolation - but that biology cares about structure and organization, not just concentrations.
APOE, triglycerides, and why genotype matters
This is where the Alzheimer’s conversation becomes unavoidable.
Astrocytes - the brain’s lipid managers- use APOE to traffic lipids. Under lipogenic conditions, APOE itself associates with lipid droplets. When APOE is dysfunctional, lipid droplet handling changes.
Astrocytes expressing APOE4, in particular, form lipid droplets that are more vulnerable to oxidative damage and impaired turnover. That suggests lipid containment and buffering may already be compromised in APOE4 brains.
So what happens if we push triglycerides aggressively lower - without regard to cellular lipid handling?
We don’t fully know. But we should at least pause.
The APOE2 paradox (and why it should make us think)
Here’s a fact that surprises many people:
APOE2 is the most protective genotype for Alzheimer’s disease risk.
And yet - APOE2 homozygotes (2/2) are also the group most prone to elevated triglycerides and delayed remnant clearance.
I stumbled onto this while analyzing my APOE2/2 husband’s lipid profile. His triglycerides consistently run higher, increasing his cardiovascular risk, yet his genetics are strongly protective against Alzheimer’s disease.
That does not mean high triglycerides are beneficial. It means the relationship between triglycerides, lipid trafficking, and brain health is not linear.
If the genotype most protective against Alzheimer’s tends to tolerate - or even trend toward - higher triglycerides, then blanket claims that triglycerides should be driven as low as possible for everyone deserve closer scrutiny.
Context matters. Genetics matters. Mechanism matters.
And yes - as a 4/4 myself, I did manage one major strategic win: choosing a 2/2 husband to offset our children’s AD risk. A rare gem indeed - only about 0.5–1% of the population.
Genetics is humbling… but not entirely without humor and irony.
When low triglycerides may actually be a signal
Several large observational studies in older adults have shown something deeply unfashionable:
Very low triglycerides are associated with higher dementia risk
In the “oldest old,” higher triglycerides correlate with lower risk of cognitive decline, frailty, and mortality
Low triglycerides have been associated with increased hemorrhagic stroke risk
This does not mean anyone should aim to raise triglycerides. It means that in late life - or in people who are under-fueling, over-restricting, or stacking triglyceride-lowering interventions - very low triglycerides may reflect loss of metabolic reserve, not metabolic excellence.
Medicine is good at lowering numbers. It’s less good at asking what those numbers represent in context.
APOE4, DHA delivery, and lipid transport
Work by researchers like Dr. Hussein Yassine has highlighted another important point: lipid delivery to the brain differs by APOE genotype.
In DHA supplementation studies, APOE4 carriers show reduced enrichment of CSF omega-3s compared with non-carriers - suggesting transport, not intake, may be the bottleneck.
This reinforces the broader theme:
In APOE4, lipid handling matters as much as lipid levels.
Driving triglycerides ever lower without considering how lipids are trafficked, stored, and delivered - especially in the brain - may solve one problem while quietly creating another.
So what’s the sane position?
Here’s my thought:
In midlife, elevated triglycerides often reflect metabolic dysfunction and should be addressed - primarily by fixing insulin resistance, not just suppressing the number.
In later life, very low triglycerides can be a warning sign of under-fueling, frailty, or diminished resilience.
For APOE4, lipid organization and delivery may matter more than achieving textbook-perfect fasting values.
Biology rarely rewards extremes.
When might triglycerides be “too low”?
There is no universally agreed cutoff - but observational studies linking low TG to dementia, frailty, or hemorrhagic stroke often involve fasting triglycerides below ~60 mg/dL, and sometimes below 50 mg/dL, particularly in older adults.
Low triglycerides deserve a second look when they coexist with:
unintentional weight loss or sarcopenia
aggressive carbohydrate or fat restriction
excessive fasting in older age
fatigue, poor sleep, cold intolerance
low insulin, low leptin, or other signs of under-fueling
This is not a call to raise triglycerides.
It is a call to stop celebrating low numbers without context.
Closing thought
Triglycerides are not merely a risk marker to be crushed into submission. They are part of the system that keeps lipids organized, contained, and less toxic - both in plasma and inside cells.
If APOE2 homozygotes can carry higher triglycerides yet enjoy the lowest Alzheimer’s risk, that alone should make us skeptical of one-size-fits-all lipid dogma.
Analysis is correct. Context is everything. Situational analysis is always key to the optimun practice of medicine.
This was a really valuable read. I appreciate you sharing it.